The Luria three-step motor sequence — fist, edge, palm, repeated in smooth succession — is one of the oldest and fastest bedside probes of frontal-lobe programming still in routine use. It takes seconds to administer. Scoring it well, while it’s happening in front of you, is the harder part.
What the sequence actually measures
The test asks a patient to perform a simple three-position hand sequence, repeating it fluently without cueing. What you’re watching for isn’t dexterity — it’s the ability to program and execute a novel motor sequence and then run it automatically. That’s a function of the prefrontal cortex, particularly the dorsolateral and supplementary motor regions, working alongside the basal ganglia to convert a learned sequence into smooth, self-sustained output.
Breakdown shows up in a small number of recognisable ways: perseverative errors (repeating a position instead of moving to the next), sequencing errors, hesitations between elements, and outright freezes where the patient loses the motor plan mid-sequence. Each of these is informative, and each is easy to miss if you’re trying to count them live while also managing the rest of the encounter.
Why it matters clinically
The Luria sequence is a quick, sensitive marker of executive motor dysfunction — it’s part of the classic bedside battery for frontal lobe function, alongside tasks like go/no-go and alternating sequences. A patient who cascades into perseveration or freezes repeatedly is showing you something about programming and inhibitory control that a strength or reflex exam won’t.
It shows up across a wide range of presentations: post-traumatic brain injury follow-up, workup for suspected frontotemporal or subcortical neurodegenerative disease, and monitoring recovery through a course of neurorehabilitation. Because it’s quick to repeat, it’s also genuinely useful longitudinally — a consistent, comparable measure you can revisit at review rather than a one-off impression.
The clinically useful signal usually isn’t just “pass or fail” — it’s the specific pattern of errors, freezes and hesitations, and whether that pattern is improving or worsening across visits.
The problem with scoring it live
Here’s the practical friction: tallying successes, errors, freezes and hesitations accurately while the sequence is running in real time is genuinely difficult, especially at normal conversational pace. Attention split between administering the test, managing the patient, and counting subtle motor breakdowns means detail gets lost — particularly the difference between a brief hesitation and a true freeze, which matters more than it sounds.
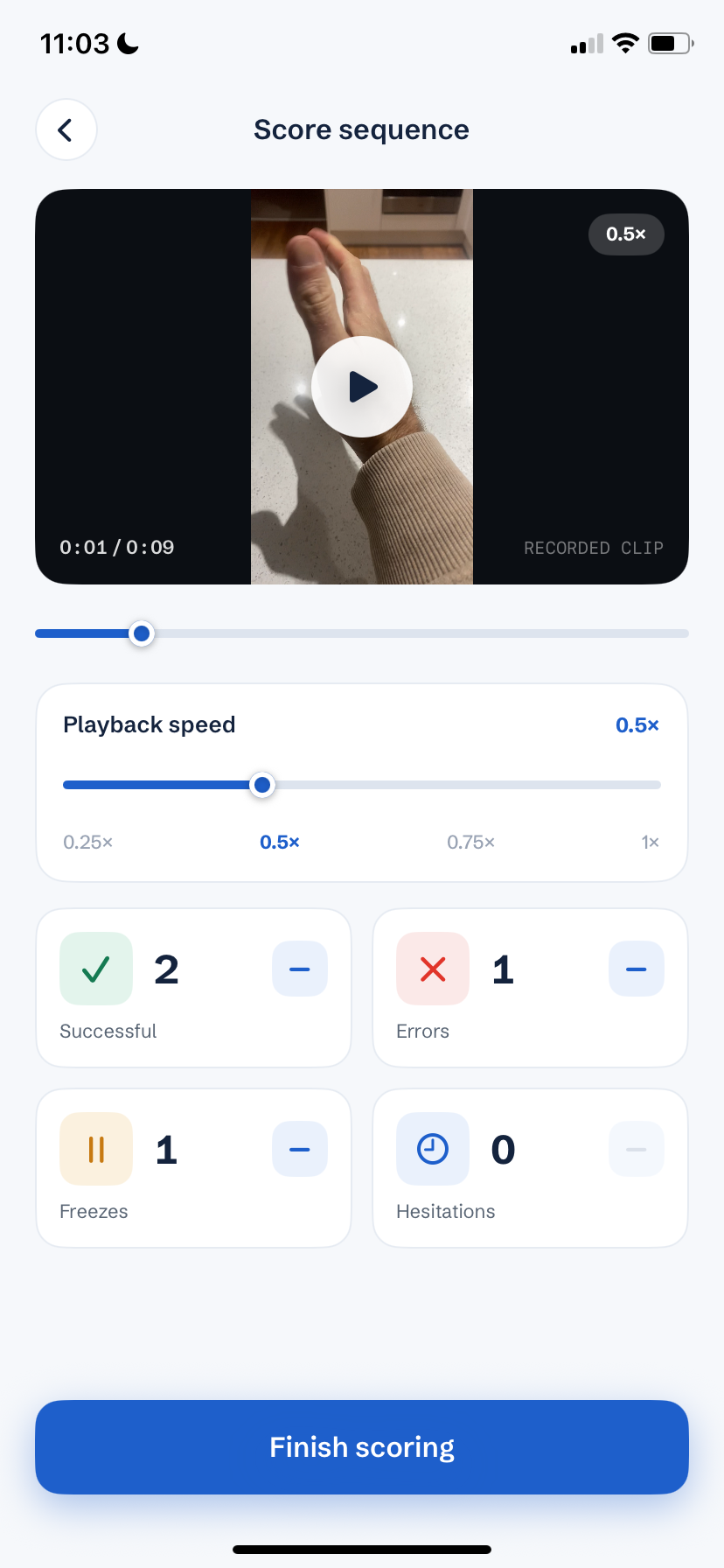
Recording the test removes that trade-off entirely. Instead of scoring on the fly, you capture the whole sequence uninterrupted, then replay it afterwards — in slow motion if needed — to score calmly and consistently. That’s the exact gap Luria Sequencing is built to close: point an iPhone at the patient’s hands, record the full assessment, then review and tally each error type at your own pace before saving the result to the record. It doesn’t interpret anything for you — it just gives you an accurate, reviewable record of what happened, with the video never leaving the device.
Fitting it into a routine exam
A simple, repeatable protocol:
- Position the camera to frame the patient’s hands clearly on the table, with nothing else needed.
- Ask the patient to perform the fist-edge-palm sequence, repeated smoothly, without interruption.
- Record the entire attempt rather than stopping and restarting — breakdowns are part of the data.
- Review the clip afterwards and tally successes, errors, freezes and hesitations against your own criteria.
- Note the pattern alongside your other findings, so you have something concrete to compare at the next review.
Done this way, a test that’s almost too fast to score properly in the room becomes a calm, repeatable measure — one you can trust to be consistent from visit to visit, and from clinician to clinician.
This article is general clinical education and isn't a substitute for formal training or guidelines. Always interpret bedside tests in the context of the full examination.